- Research article
- Open access
- Published:
Family satisfaction in the intensive care unit, a cross-sectional study from Norway
BMC Emergency Medicine volume 21, Article number: 20 (2021)
Abstract
Background
Becoming critically ill represents not just a great upheaval for the patient in question, but also for the patient’s closest family. In recent years, there has been a change in how the quality of the public health service is measured. There is currently a focus on how patients and their families perceive the quality of treatment and care. It can be challenging for patients to evaluate their stay in an intensive care unit (ICU) due to illness and treatment. Earlier studies show that the perceptions of the family and the patient may concur. It is important, therefore, to ascertain the family’s level of satisfaction with the ICU stay.
The aim of the study was to describe how the family evaluate their satisfaction with the ICU stay. A further aim was to identify which demographic variables were associated with differences in family satisfaction.
Method
The study had a cross-sectional design. A sample of 57 family members in two ICUs in Norway completed the questionnaire: Family satisfaction in the intensive care unit 24 (FS-ICU 24). Statistical analysis was conducted using the Mann-Whitney U test (U), Kruskal Wallis, Spearman rho and a performance-importance plot.
Results
The results showed that families were very satisfied with a considerable portion of the ICU stay. Families were less satisfied with the information they received and the decision-making processes than with the nursing and care performed during the ICU stay. The results revealed that two demographic variables – relation to the patient and patient survival – significantly affected family satisfaction.
Conclusion
Although families were very satisfied with the ICU stay, several areas were identified as having potential for improvement. The results showed that some of the family demographic variables were significant for family satisfaction. The findings are clinically relevant since the results can strengthen intensive care nurses’ knowledge when meeting the family of the intensive care patient.
Background
Intensive care units (ICUs) are highly technological wards where critically ill patients receive treatment, nursing and care. The reasons for admission to intensive care are many and complex. The patient’s recollections of the ICU stay may consist of unclear memories and hallucinations caused by ICU delirium as well as actual events [1,2,3]. Studies show that patients can develop post-intensive care syndrome (PICS) as a result of the ICU stay [4, 5].Becoming critically ill represents not merely a great upheaval for the patient but also for their close family. Family members play a key role as both mediators of the intensive care patient’s needs and wishes and as a health-promoting resource that can improve patient outcomes [6, 7]. Family members’ needs and wishes are important in terms of both their role as supporters for the patients, and their own personal needs. Studies show that there may be a high prevalence among family members of depression, post-traumatic stress disorder (PTSD) or PICS-Family at the end of an ICU stay [8, 9].
Many families experience the time spent in the ICU as challenging [10, 11] and full of uncertainty regarding the intensive care patient’s condition, treatment and prognosis [12]. Family members describe the experience and the sight of the intensive care patient as well as the surroundings of the hospital bed, as frightening and unreal [13, 14]. They want to participate in patient care [7, 10] and be included in decision-making processes [12, 15]. Dodek et al. [16] and Wall et al. [17] claim that there is a potential for improvement in respect of the family’s perceptions of receiving support in the decision-making processes. Information exchanges where the ICU nurse is not present can make further communication between them and the family members more difficult [15, 18, 19]. Nevertheless, family members describe the support they receive from the ICU nurses as crucial for them in coping with the situation and understanding what is happening [12, 14].
In recent years, the patient’s perceptions of quality of care or satisfaction and the views of their family have been highlighted and used as one of several internationally recommended quality indicators for intensive care medicine [20, 21]. Donabedian [22] asserts that client satisfaction is very important as a measurement of the quality of medical services and provides information about whether health personnel have successfully responded to the client’s values and expectations. However, on account of their illness and treatment, it can be challenging for patients to evaluate the ICU stay [23]. Studies show that the patient’s and the family’s perception of an ICU stay can be the same [24,25,26]. In recent years, knowledge about the experiences of the patient and their family during the ICU stay has resulted in increased research on family satisfaction [6, 27, 28].
Family satisfaction with the care received by the patient during an ICU stay can be an important piece of information used in overall ICU quality enhancement, ensuring that the care provided meets both the patient’s and the family’s needs [29]. Few quantitative studies on family satisfaction following an ICU stay have hitherto been published in Norway. More knowledge is vital for both safeguarding the needs of family members and for assessing transferability between national and international research. It is also important to investigate how different demographic variables affect family members’ satisfaction ratings.
The aim of the study was to describe how family members assessed their satisfaction with the ICU stay using the Family Satisfaction in the Intensive Care Unit 24 (FS-ICU 24) questionnaire. Another aim was to identify which demographic variables were associated with differences in family satisfaction.
Methods
Design
The study had a cross-sectional design.
Setting
The hospitals with the two ICUs included in the study were located in medium-sized towns in Norway with a population of just over 30,000 [30]. The two ICUs had a comparable catchment area, level of treatment, and both medical and surgical intensive care patients. The ICUs had a nurse-to-patient ratio of 1:1–2 and a senior consultant in anaesthesiology in 24-h attendance. Both ICUs had family waiting rooms that family members could use when not accompanying the ICU patient. The two ICUs had an equal number of visiting hours and a clear policy of welcoming relatives within their units. However, there were no written guidelines about caring for the relatives.
Participants
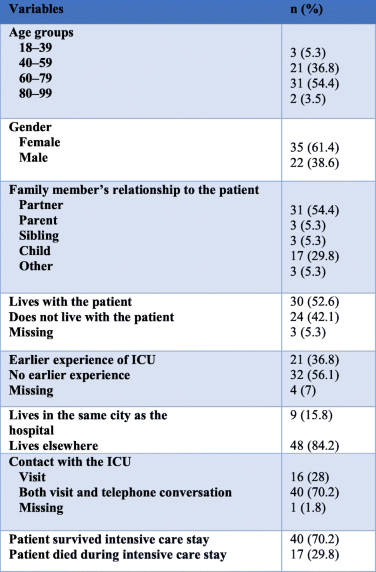
Participants included family members, aged 18 and over, of ICU patients hospitalized for more than 48 h or, family members of patients who had died in the ICU. Other inclusion criteria were ability to read and write Norwegian and registered as the main family member (only one per patient) in the patient record. The family members were aged between 29 and 85 year with a mean age of 59.9 years and 61% were women (Table 1).
Data collection
The Norwegian Intensive Care Registry (NICR) and the Centre for Clinical Documentation and Evaluation (CCDE) carried out a Family Satisfaction in the Intensive Care Unit (FSICU) project from 2015 to 2017 in order to map out family satisfaction [31], but the data has not yet been published. The present study makes use of baseline data (October–December 2015) obtained in two of the ICUs that participated in the FSICU project. Three weeks after the ICU stay, the FS-ICU 24 questionnaire, an information letter and a prepaid envelope were sent to the main family members that met the inclusion criteria. Family members did not receive any information about the project during the ICU stay and no identifying data were included in the questionnaires so that family members could remain anonymous. Returned questionnaires were considered as written informed consent. Family members of patients with several ICU stays during the period of the study were only included once. Altogether, 165 questionnaires were distributed, of which 65 (39.4%) were returned. Eight of the questionnaires returned were excluded because they had > 30% missing values [32]. A total of 57 (34.5%) questionnaires were included in the study. The number of returned questionnaires by family members was approximately the same for both ICUs (27/47.4% versus 30/52.6%). The two groups of family members (one from each ICU) did not differ with regards demographic variables.
The FSICU project, under the auspices of NICR, was approved by the Norwegian Data Protection Authority [31]. NICR and the data protection officer at the hospitals gave written permission to use the data material in this study and considered that no other formal ethical approval was required.
Questionnaire
The FS-ICU 24 questionnaire measures family satisfaction with the care given to the patient and their family during the ICU stay. The questionnaire is a further development of the original FS-ICU 34 version, devised by the Kingston General Hospital ICU Research Working Group [33]. The FS-ICU 24 has good psychometric properties [34, 35]. It has been translated to a number of languages and is used in many international studies [36,37,38]. The FS-ICU 24 includes the FS-Total score, FS-Care and FS-Decision making (DM) subscales, with responses on a Likert scale from 1 to 5, where 1 is poor and 5 is excellent [39]. In addition, the questionnaire contains demographic questions and three open-ended questions where family members can write free-text comments. The FS-ICU 24 was translated into Norwegian and back translated to English in line with the World Health Organization’s guidelines [40, 41], but has not yet undergone validity and reliability testing in Norway.
Analysis
Data was systematized according to the procedure for recoding and scoring of FS-ICU 24 questionnaire [32]. The procedure describes recoding from Likert scale 1–5 to a new scale with score 0–100, where 0 = poor, 25 = fair, 50 = good, 75 = very good and 100 = excellent. Missing values < 30% were imputed using the individual family member’s mean value for the relevant subscale.
The Mann-Whitney U test (U) was used to examine whether there were any differences between family satisfaction on items, subscales and total score and the family’s demographic variables when there were two independent samples. In respect of two of the demographic variables – family member’s age and relationship to the patient – we chose to dichotomise the data material. The Kruskal Wallis test was used to analyse the age groups. Spearman rho was used to find the correlation coefficient between all the items in the questionnaire and overall satisfaction (FS-Total). A correlation analysis was performed with a performance-importance plot, where each individual point represented a specific item in the FS-ICU 24 questionnaire. All tests were two-tailed and the p-value p < 0.05 was regarded as statistically significant. The Statistical Package for Social Sciences (SPSS 24) was used.
Results
Patient satisfaction in the ICU
FS-care subscale
In FS-Care, family members reported on how they perceived patient treatment at the ICU and whether they themselves felt they were looked after (Table 2). The subscale showed that they were mostly very satisfied with how they and the intensive care patient were looked after. The item related to pain gained the highest mean score in terms of satisfaction. The three items – treating the patient with courtesy, respect and compassion, treating the family member with courtesy, respect and compassion and the nurses’ care for the patient – also received a high score (Table 2). The attention physicians attributed to the patient received the second lowest score whereas the lowest score was attributed to the atmosphere in the waiting room.

The FS-DM subscale
The FS-DM subscale ascertains the degree of family satisfaction with the information and decision-making process throughout the ICU stay (Table 2). Family members attributed lower scores in this subscale than in that pertaining to FS-Care. The item with the highest score in FS-DM was family members’ perceptions of having sufficient time to express their concerns and receive answers to their questions. The response distribution of this item, with two alternative responses, showed that 73.7% found that they had enough time while 26.3% would have liked to have had more time to express their concerns and obtain answers to their questions (Table 2). The willingness of ICU staff to answer family member’s questions was also highly rated. The family’s perceived control over the treatment received by the patient showed the next to lowest score whereas the lowest score, both in the FS-DM and in the study as a whole, was how frequently physicians spoke to the family.
FS-Total
The overall satisfaction of family members (FS-Total) indicated that family satisfaction was very good (Table 2).
Demographic variables and family satisfaction
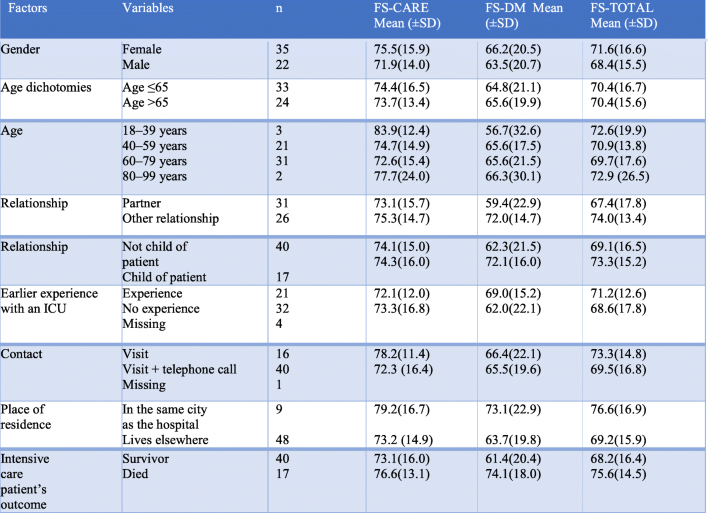
The following demographic variables were acquired: family member’s gender, age, relationship to patient, experiences of earlier ICU stays, contact with the ICU, place of residence, and the patient’s survival or death, were analysed in order to determine whether they might be associated with differences in family satisfaction.
There was little variation amongst the different demographic variables for the FS-Care subscale. The youngest family members (18–39 years) scored highest, followed by family members living in the town where the hospital was located. Males had the lowest score.
Family satisfaction scores were lower for all demographic variables in the FS-DM subscale compared to the FS-Care subscale. The families of those who died during their ICU stay had the highest score whereas those in the youngest family member group [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] had the lowest. The next to lowest score was given by the partners of ICU patients.
Family who lived in the same town as the hospital had the highest overall satisfaction (FS-Total). The families of patients who died during their ICU stay had the next highest overall satisfaction score. Family members who were partners of the intensive care patient had the lowest overall satisfaction score (Table 3).
No demographic variable attained statistical significance in the FS-Care subscale. The FS-DM subscale however did contain two significant findings. The first was the partner variable, attaining a statistical significance of p = 0.26 (Table 4) where family members in a relationship other that of partner were more satisfied (Table 3). The finding resulted in an effect size (r) of 0.296, indicating a small to medium effect (Table 4). The second variable attaining statistical significance, p = 0.01, was that concerning ICU survival (Table 4). Families of patients who died during their ICU stay had a higher satisfaction score in this subscale than those from families of patients who survived the ICU stay (Table 3). The effect size (r) of 0.343 indicated a medium effect (Table 4). No statistically significant differences were observed between the above demographic variables and the overall satisfaction score (FS-Total).

The result of the Kruskal Wallis analysis of family members’ age groups and FS-ICU 24 subscales and overall satisfaction showed that there were no significant differences.
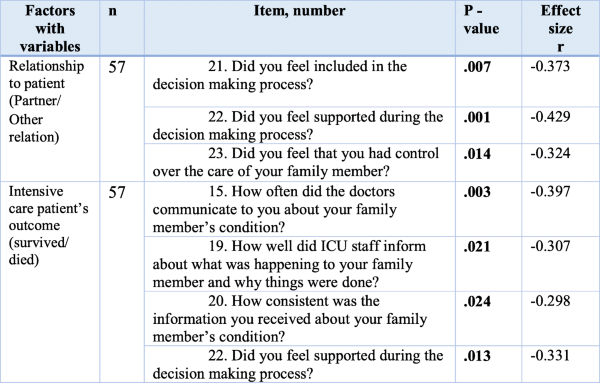
Table 5 presented the items that showed a statistical significance in relation to the various demographic variables. Family members who were not the patient’s partner were significantly more satisfied with inclusion (p= .007), control (p= .014) and support in decision-making processes (p= .001) than family members who were partners. The patient’s survival or death during the ICU stay also had significance for family satisfaction. The family of intensive care patients who died during the ICU stay were significantly more satisfied with how often the physician talked to them about the patient’s condition (p= .003), how well they were kept informed about what was happening to the patient (p= .021), consistency in the information given (p= .024), and support in the decision-making process (p= .013) (Table 5).
Correlation between items in the FS-ICU 24 questionnaire and overall satisfaction
The possible association between the FS-ICU 24 items and overall satisfaction (FS-Total) was examined using a performance-importance plot (Fig. 1).
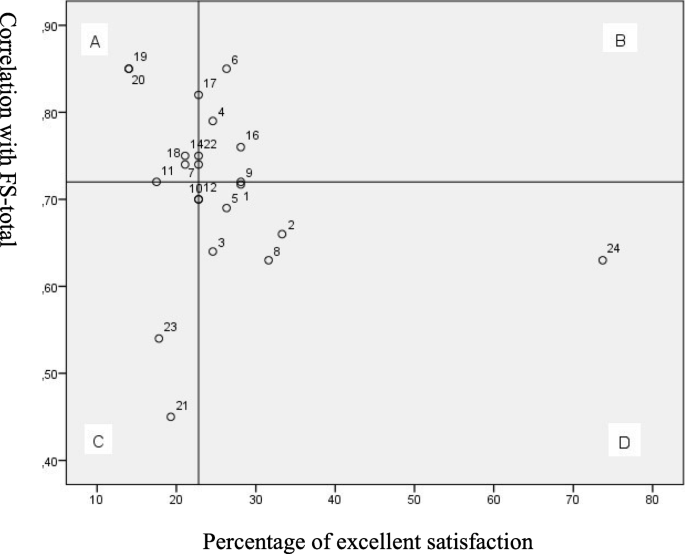
Performance-importance plot for overall satisfaction (FS-Total)
Quadrant A represents the items rated by the family members as excellent that were also highly correlated with the FS-Total. Items 19 and 20 stood out in this respect and these items concerned how well family members were informed about what was happening to the patient and the degree of consistency in the information provided by the ICU staff. For each of the items, only eight family members (14%) responded ‘excellent’. The other items in quadrant A concerned honest and understandable information, collaboration between ICU staff, the attention physicians paid, the scope of the treatment and support in decision-making.
Discussion
Our data suggests that family members were generally satisfied with the care that was received in the ICU. Family members were equally satisfied with the nursing care and with the overall treatment (FS-Care), for both the hospitalized patient and for the family itself. The degree of satisfaction was somewhat lower in relation to the information given by ICU staff, and family member’s participation in the decision-making process (FS-DM). Our results also showed that two demographic variables, a family relationship other than that of partner and, families of patient who died during their ICU stay, were associated with a high degree of satisfaction. Two items of the FS-ICU 24 questionnaire, obtaining complete and consistent information, were highly correlated with overall satisfaction, although a low percentage of family members assessed these items as excellent.
Family satisfaction in the ICU
The FS-care subscale
The FS-Care subscale showed a higher degree of satisfaction by family members than the FS-DM subscale. Earlier international studies that have used FS-ICU 24 report similar findings [36, 42,43,44].
Both ICUs had waiting/family rooms and family members assessed their satisfaction with the atmosphere in them as being considerably lower than for the other items of the FS-Care subscale. Similar findings have been reported in prior studies where the FS-ICU 24 questionnaire was used [43, 45, 46]. Engström and Söderberg [13] reported that family members greatly appreciated this room as it gave them the opportunity to step back while remaining close to the ICU patient. In contrast, other studies [11, 14] have reported that the time spent in the waiting room is perceived as stressful as family members would rather be with the patient. In addition, the limited facilities that these rooms provide are described in several studies in either a negative fashion or, as areas for potential improvement [18, 19, 25, 47].
Low satisfaction with either pain or agitation relief has been reported in several earlier studies where FS-ICU 24 was utilised [37, 43, 45, 47]. During an ICU stay, many patients develop delirium, which can cause agitation and confusion [48, 49]. It can be frightening and difficult for the family to see that their loved ones are in pain and that there is a change in their mental status. In contrast, our data suggests that family members rated their satisfaction with symptom relief as very good. There may be several reasons for this divergence. First, there may be country specific variations regarding symptom relief in the ICU [50] and second, an increased focus on analgosedation in Norwegian ICUs [51]. Nevertheless, Woien, Stubhaug and Bjork [52] found that practices between Norwegian ICUs vary and this may result in family members assessing symptom relief differently. Differences in symptom treatment should therefore be stressed when comparing the results of studies.
The FS-DM subscale
Our data suggests that family member’s satisfaction, as measured by the FS-DM subscale, was lower than that reported in earlier research using the same questionnaire in Canada [16], Norway [42], Germany [47] and the USA [53, 54].Family members assessed their satisfaction with the frequency of conversations with physicians as low. They expected to receive accurate and unfiltered information, even in the event of bad news [12, 13]. Dodek et al. [16], Lind et al. [15] and Wall et al. [17] suggested that family members had a low level of satisfaction with the frequency of conversations with physicians. However, the structure of the FS-DM subscale does not provide information as to the actual content of the conversation or, whether family members felt the need to talk to physicians more often than was the case. Whether family member’s response would have been different had the question been formulated differently, for example: ‘Did you receive adequate information from the physician?’ It is arguable whether frequent conversations always result in a higher degree of satisfaction or whether the content of and access to information from the intensive care staff are the most important. All patient situations are different and the need for information will vary. The family members’ perceptions of a lack of information may be because they did not understand or had not received the information they wanted, as described by Frivold, Dale and Slettebo [12] and Lind et al. [15]. Another reason may be that they did not remember the information they had been given due to the gravity of the situation.
Family satisfaction with the time available for getting answers to their questions and the willingness of intensive care staff to reply to these questions was rated as highest in the FS-DM subscale. The results were somewhat surprising since family members rated the frequency of conversations with physicians as the item with lowest satisfaction. This finding suggests that it may be ICU nurses who primarily answer many of the family’s questions. The family’s need for information about the intensive care patient’s condition, care and treatment is highlighted in a number of earlier studies [13, 18, 19, 47]. As reported by Agard and Harde’s [11] family members express the need to obtain information throughout the entire care pathway, including when intensive care staff have no new information to impart.
FS-Total
Although our results show that family members rated overall satisfaction with the ICU stay as high this rating was nevertheless lower than earlier research using FS-ICU 24 [16, 33, 35,36,37, 43, 44, 47, 53,54,55].
In research on people’s perceptions and satisfaction, it would be impossible and unrealistic to expect that everyone is completely satisfied with all the situations they experience [56]. Donabedian [57] states that quality demands can never be completely satisfied. Earlier studies also examined the term ‘complete satisfaction’ and raised the question of what the goal for family satisfaction should be [27, 37]. Donabedian [22] points out that family expectations and needs will not always be realistic and feasible, which may affect their perceptions of satisfaction. Family members’ limited knowledge about medical treatment and intensive care technical equipment may give them unrealistic expectations, which in turn may affect their satisfaction.
Demography and family satisfaction
Our results showed that partners were less satisfied than family members with no marital relationship with the patient. Conversely, other researchers found no association between satisfaction and the relationship between patient and family member [25, 47, 58]. On the other hand Hunziker et al.’s [45] reported that family members who did not live together with the patient were more likely to be dissatisfied with the ICU stay, but their relationship with the patient was not further specified. The statistically significant results at item level concerned the role of family members in decision-making processes in the form of support, inclusion and control. Differences in family satisfaction based on relationships may be associated with family members’ varying expectations. Partners may have different wishes and needs in the decision-making process than other family members.
Our results showed that the families of patients who died expressed greater satisfaction overall and, in both subscales (FS-DM and FS-Care) used in this study. A number of international studies that have used FS-ICU 24 have investigated whether ICU survival has significance for family satisfaction, although the findings vary. The results of Dodek et al.’s [16] study showed that the family of patients who die rate their satisfaction with the decision-making process as higher. Pagnamenta et al. [36] and Wall et al. [17] found greater satisfaction in all subscales among the family members of patients who died. Other studies found no correlation between the survival of the intensive care patient and family satisfaction [43, 45, 47].
There may be several reasons why the family of patients who died during the ICU stay were more satisfied. Wall et al. [17] stated that the results do not indicate that the families of those who die received better care, but that they may indicate that healthcare personnel make an extra effort to meet family members’ wishes as death approaches. The results in this study showed that the families of those who died rated their satisfaction with the frequency of conversations with the physician and information about patient treatment significantly higher. These family members were also more satisfied with the consistency of the information provided and the support they received during the decision-making processes. The ICUs in this study did not have a standardised follow-up of relatives of patients who died during the stay. The intensive care staff in the wards nevertheless had an established tradition of meeting the needs of the family members.
Association between the items of the FS-ICU 24 questionnaire and overall satisfaction
One of the main aims of measuring family satisfaction was to map this and be able to use the findings in quality improvement work [59]. The results of the performance-importance plot revealed several items that have a high correlation with overall family satisfaction, but which a small percentage of family members rated as excellent. There are two items in particular that stood out in the plot, both of which belonged to the FS-DM subscale. These two items concerned how well family members were informed about what was happening to the patient and the degree of consistency in the information given. Other international studies using FS-ICU 24 reported similar findings [36, 37]. Family members express frustration over the lack of continuity in the healthcare personnel around the patient, which makes it difficult for them to keep up with the treatment plans and contribute to the decision-making processes [18]. Schwarzkopf et al. [47] reported similar findings, where family members stated that there were many physicians with different opinions throughout the course of the ICU stay. Continuity among the healthcare team surrounding the patient can help to give family members accurate and consistent information about what is happening to the patient. The results of the performance-importance plot were useful in the quality improvement work at the two included ICUs as well as forming a basis for comparison for other studies that focus on how relatives' satisfaction can be strengthened.The lack of consistent information may indicate a lack of coordination in how ICU personnel provide this information to the families. The intensive care nurse plays an important role in supporting the family and imparts a sense of security [12]. Conversely, intensive care nurses can sometimes be regarded as vague and evasive when communicating the patient’s prognosis and risk, since these conversations often take place around the patient’s bed and are limited to the monitoring of vital signs [60]. Family members can perceive information from physicians as more honest and complete than information from the intensive care nurses [47]. The Norwegian intensive care nurse’s limited scope to inform family members about treatment and prognoses may be one of the reasons why family members rated consistency of information as low [61]. The results of this study show that it is vital that family are adequately informed such that they understand the information they receive about the patient’s condition, treatment and prognosis.
Strengths and limitations
FS-ICU 24 is a well-validated and reliability-tested questionnaire that has been translated into several languages and used in many countries [35, 38]. One strength of this study is that the FS-ISU 24 questionnaire has good psychometric properties, while a weakness is that the Norwegian version of the questionnaire has not been validated and tested for reliability. The data material contains no details about the patient’s background information or the severity of the illness, which is a weakness in this study. The study has a small sample size and a predominance of female respondents. Small sample size is a well-known weakness in this field of research [36, 47, 54], and can cause biases that affect the possibility of generalization to other ICUs nationally and internationally. Nevertheless, this article is one of very few studies that present results from a Norwegian setting. Furthermore, it is important to gain knowledge about relatives' satisfaction with the ICU.
The study’s performance-importance plot clearly indicates areas where measures can be implemented to increase overall satisfaction with the ICU stay. According to Dodek et al. [59], quality enhancement is a key goal when charting family satisfaction and the plot therefore represents a strength for the study’s clinical relevance. Another strength is that the results of the plot can be compared with findings from other performance-importance plots conducted in international studies that have utilised FS-ICU 24.
Conclusion
The results showed that families were very satisfied with a large portion of the ICU stay, but that there was a potential for improvement in relation to how well the family members were informed about what was happening to the patient and the degree of consistency in the information given by intensive care staff. The results also showed that the family members’ relationship to the intensive care patient and the intensive care patient’s outcome may be significant for the degree of satisfaction. The findings have clinical relevance since they indicate that different patient care pathways and different family/patient relationships may require different types of follow-up and involve different needs during the ICU stay. Involvement and the safeguarding of family members in an ICU entail work based on traditions, culture and knowledge. The results of the study may help to provide intensive care nurses with balanced knowledge that can increase their competence when they meet the families of intensive care patients. The results may also be of importance for hospital management and other political decision-makers in their work on quality enhancement and service development.
There is a need for more studies with a larger sample and studies to test the psychometric properties of the Norwegian version of FS-ISU 24.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- FS-Care:
-
Family satisfaction care
- FS-DM:
-
Family satisfaction decision-making
- FS-Total:
-
Family satisfaction total
- FSICU:
-
Family Satisfaction in the Intensive Care Unit project
- FS-ICU 24:
-
Family Satisfaction in the intensive care unit 24
- ICU:
-
Intensive care unit
- NICR:
-
Norwegian Intensive Care Registry
- PICS:
-
Post-intensive care syndrome
- PICS-Family:
-
post-intensive care syndrome – family
- PTSD:
-
Post-traumatic stress disorder
- CCDE:
-
Centre for Clinical Documentation and Evaluation
- SPSS 24:
-
Statistical Package for Social Sciences
- WHO:
-
World Health Organization
References
Jones C. Recovery post ICU. Churchill: Livingstone; 2014. p. 239–45.
Olsen KD, Nester M, Hansen BS. Evaluating the past to improve the future – a qualitative study of ICU patients’ experiences. Intens Crit Care Nurs. 2017;43:61–7. https://doi.org/10.1016/j.iccn.2017.06.008.
Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–16. https://doi.org/10.1056/NEJMoa1301372.
Elliott D, Davidson JE, Harvey MA, Bemis-Dougherty A, Hopkins RO, Iwashyna TJ, et al. Exploring the scope of post-intensive care syndrome therapy and care: engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit Care Med. 2014;42(12):2518-26. https://doi.org/10.1097/CCM.0000000000000525.
Marra A, Pandharipande PP, Girard TD, Patel MB, Hughes CG, Jackson JC, et al. Co-occurrence of post-intensive care syndrome problems among 406 survivors of critical illness. Crit Care Med. 2018;46(9):1393–401. https://doi.org/10.1097/CCM.0000000000003218.
Davidson JE, Aslakson RA, Long AC, Puntillo KA, Kross EK, Hart J, et al. Guidelines for family-centered Care in the Neonatal, pediatric, and adult ICU. Crit Care Med. 2017;45(1):103–28. https://doi.org/10.1097/CCM.0000000000002169.
Haugdahl HS, Eide R, Alexandersen I, Paulsby TE, Stjern B, Lund SB, et al. From breaking point to breakthrough during the ICU stay: a qualitative study of family members’ experiences of long-term intensive care patients’ pathways towards survival. J Clin Nurs. 2018;27(19–20):3630–40. https://doi.org/10.1111/jocn.14523.
Davidson JE, Jones C, Bienvenu OJ. Family response to critical illness: postintensive care syndrome-family. Crit Care Med. 2012;40(2):618-24. https://doi.org/10.1097/CCM.0b013e318236ebf9.
van Beusekom I, Bakhshi-Raiez F, de Keizer NF, Dongelmans DA, van der Schaaf M, et al. Crit Care. 2016;20(1). https://doi.org/10.1186/s13054-016-1185-9.
Blom H, Gustavsson C, Sundler AJ. Participation and support in intensive care as experienced by close relatives of patients: a phenomenological study. Intens Crit Care Nurs. 2013;29(1):1–8. https://doi.org/10.1016/j.iccn.2012.04.002.
Agard AS, Harder I. Relatives' experiences in intensive care--finding a place in a world of uncertainty. Intens Crit Care Nurs. 2007;23(3):170–7. https://doi.org/10.1016/j.iccn.2006.11.008.
Frivold G, Dale B, Slettebo A. Family members' experiences of being cared for by nurses and physicians in Norwegian intensive care units: a phenomenological hermeneutical study. Intens Crit Care Nurs. 2015;31(4):232–40. https://doi.org/10.1016/j.iccn.2015.01.006.
Engstrom A, Soderberg S. The experiences of partners of critically ill persons in an intensive care unit. Intens Crit Care Nurs. 2004;20(5):299–308; quiz 9-10.doi:https://doi.org/10.1016/j.iccn.2004.05.009.
Nelms TP, Eggenberger SK. The essence of the family critical illness experience and nurse-family meetings. J Fam Nurs. 2010;16(4):462–86. https://doi.org/10.1177/1074840710386608.
Lind R, Lorem GF, Nortvedt P, Hevroy O. Family members' experiences of "wait and see" as a communication strategy in end-of-life decisions. Intens Care Med. 2011;37(7):1143–50. https://doi.org/10.1007/s00134-011-2253-x.
Dodek PM, Wong H, Heyland DK, Cook DJ, Rocker GM, Kutsogiannis DJ, et al. The relationship between organizational culture and family satisfaction in critical care. Crit Care Med. 2012;40(5):1506–12. https://doi.org/10.1097/CCM.0b013e318241e368.
Wall RJ, Curtis JR, Cooke CR, Engelberg RA. Family satisfaction in the ICU: differences between families of survivors and nonsurvivors. Chest. 2007;132(5):1425–33. https://doi.org/10.1378/chest.07-0419.
Hansen L, Rosenkranz SJ, Mularski RA, Leo MC. Family perspectives on overall Care in the Intensive Care Unit. Nurs Res. 2016;65(6):446–54. https://doi.org/10.1097/NNR.0000000000000179.
Henrich NJ, Dodek P, Heyland D, Cook D, Rocker G, Kutsogiannis D, et al. Qualitative analysis of an intensive care unit family satisfaction survey. Crit Care Med. 2011;39(5):1000–5. https://doi.org/10.1097/CCM.0b013e31820a92fb.
Murphy DJ, Ogbu OC, Coopersmith CM. ICU director data: using data to assess value, inform local change, and relate to the external world. Chest. 2015;147(4):1168–78. https://doi.org/10.1378/chest.14-1567.
Hinkle LJ, Bosslet GT, Torke AM. Factors associated with family satisfaction with end-of-life care in the ICU: a systematic review. Chest. 2015;147(1):82–93. https://doi.org/10.1378/chest.14-1098.
Donabedian A. The definition of quality and approaches to its assessment. Ann Arbor: Health Administration Press; 1980. xiii, 163 p. p.
Burry L, Cook D, Herridge M, Devlin JW, Fergusson D, Meade M, et al. Recall of ICU stay in patients managed with a sedation protocol or a sedation protocol with daily interruption. Crit Care Med. 2015;43(10):2180–90. https://doi.org/10.1097/CCM.0000000000001196.
Holanda Pena MS, Talledo NM, Ots Ruiz E, Lanza Gomez JM, Ruiz Ruiz A, Garcia Miguelez A, et al. Satisfaction in the intensive care unit (ICU). Patient opinion as a cornerstone. Med Int. 2017;41(2):78–85. https://doi.org/10.1016/j.medin.2016.06.007.
Mosleh S, Alja'afreh M, Lee AJ. Patient and family/friend satisfaction in a sample of Jordanian critical care units. Intens Crit Care Nurs. 2015;31(6):366–74. https://doi.org/10.1016/j.iccn.2015.04.004.
Stricker KH, Kimberger O, Brunner L, Rothen HU. Patient satisfaction with care in the intensive care unit: can we rely on proxies? Acta Anaesthesiol Scand. 2011;55(2):149–56. https://doi.org/10.1111/j.1399-6576.2010.02293.x.
Padilla Fortunatti C, Rojas SN. Families on adult intensive care units: are they really satisfied? A literature review. Aust Crit Care. 2018;31(5):318–24. https://doi.org/10.1016/j.aucc.2017.08.003.
Mitchell ML, Coyer F, Kean S, Stone R, Murfield J, Dwan T. Patient, family-centred care interventions within the adult ICU setting: an integrative review. Aust Crit Care. 2016;29(4):179–93. https://doi.org/10.1016/j.aucc.2016.08.002.
Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al. The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature. Health Technol Assess. 2002;6(32):1–244. https://doi.org/10.3310/hta6320.
Population Statistics Norway, ; 2020 [cited 2020 18.06]. Available from: https://www.ssb.no/en/befolkning.
Sjøbø B. Familysatisfaction in Norwegian ICUs-a quality improvement project [Norwegian] 2017 [cited 2020 19.06]. Available from: https://helse-bergen.no/seksjon/intensivregister/Documents/Forskning,%20studier/Prosjektdokument%20-%20familietilfredshet/Sluttrapport%20revidert.pdf.
Calculating summary scores for the FS-ICU 24: FSICU.org; [cited 2020 19.06]. Available from: https://fsicu.org/wp-content/uploads/New-FS-ICU24-Scoring-Instructions.pdf. Accessed 11 Feb 2021.
Heyland DK, Tranmer JE, Kingston General Hospital ICURWG. Measuring family satisfaction with care in the intensive care unit: the development of a questionnaire and preliminary results. J Crit Care. 2001;16(4):142–9. https://doi.org/10.1053/jcrc.2001.30163.
van den Broek JM, Brunsveld-Reinders AH, Zedlitz AM, Girbes AR, de Jonge E, Arbous MS. Questionnaires on family satisfaction in the adult ICU: a systematic review including psychometric properties. Crit Care Med. 2015;43(8):1731–44. https://doi.org/10.1097/CCM.0000000000000980.
Wall RJ, Engelberg RA, Downey L, Heyland DK, Curtis JR. Refinement, scoring, and validation of the family satisfaction in the intensive care unit (FS-ICU) survey. Crit Care Med. 2007;35(1):271–9. https://doi.org/10.1097/01.CCM.0000251122.15053.50.
Pagnamenta A, Bruno R, Gemperli A, Chiesa A, Previsdomini M, Corti F, et al. Impact of a communication strategy on family satisfaction in the intensive care unit. Acta Anaesthesiol Scand. 2016;60(6):800–9. https://doi.org/10.1111/aas.12692.
Stricker KH, Kimberger O, Schmidlin K, Zwahlen M, Mohr U, Rothen HU. Family satisfaction in the intensive care unit: what makes the difference? Intensive Care Med. 2009;35(12):2051–9. https://doi.org/10.1007/s00134-009-1611-4.
About the FS-ICU Survey [cited 2020 19.06]. Available from: https://fsicu.org/professionals/about/. Accessed 11 Feb 2021.
Connections CC. Family Satisfaction with Care in the Intensive Care Unit© FS-ICU (24) 2006 [cited 2020 19.06]. Available from: https://fsicu.org/wp-content/themes/fsicu/assets/files/FS-ICU-24/FS_ICU_24_EnglishCopyright.pdf.
Dybwik K. Questionnaire on relatives' satisfaction with care and treatment at intensive care unit © (FS-ICU24) [Norwegina] 2006 [cited 2020 19.06]. Available from: https://fsicu.org/wp-content/themes/fsicu/assets/files/FS-ICU-24/FS_ICU_24_NorwegianDybwikCopyright.pdf.
WHO. Process of translation and adaptation of instruments 2020 [cited 20220 19.06]. Available from: http://www.who.int/substance_abuse/research_tools/translation/en/.
Frivold G, Slettebo A, Heyland DK, Dale B. Family members' satisfaction with care and decision-making in intensive care units and post-stay follow-up needs-a cross-sectional survey study. Nurs Open. 2018;5(1):6–14. https://doi.org/10.1002/nop2.97.
Lam SM, So HM, Fok SK, Li SC, Ng CP, Lui WK, et al. Intensive care unit family satisfaction survey. Hong Kong Med J. 2015;21(5):435–43. https://doi.org/10.12809/hkmj144385.
Wright SE, Walmsley E, Harvey SE, Robinson E, Ferrando-Vivas P, Harrison DA, et al. Family-reported experiences evaluation (FREE) study: a mixed-methods study to evaluate families' satisfaction with adult critical care services in the NHS. Southampton: Health Services and Delivery Research; 2015.
Hunziker S, McHugh W, Sarnoff-Lee B, Cannistraro S, Ngo L, Marcantonio E, et al. Predictors and correlates of dissatisfaction with intensive care. Crit Care Med. 2012;40(5):1554–61. https://doi.org/10.1097/CCM.0b013e3182451c70.
Min J, Kim Y, Lee JK, Lee H, Lee J, Kim KS, et al. Survey of family satisfaction with intensive care units: a prospective multicenter study. Medicine (Baltimore). 2018;97(32):e11809. https://doi.org/10.1097/MD.0000000000011809.
Schwarzkopf D, Behrend S, Skupin H, Westermann I, Riedemann NC, Pfeifer R, et al. Family satisfaction in the intensive care unit: a quantitative and qualitative analysis. Intensive Care Med. 2013;39(6):1071–9. https://doi.org/10.1007/s00134-013-2862-7.
Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and Management of Pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e73. https://doi.org/10.1097/CCM.0000000000003299.
Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–62. https://doi.org/10.1001/jama.291.14.1753.
Patel RP, Gambrell M, Speroff T, Scott TA, Pun BT, Okahashi J, et al. Delirium and sedation in the intensive care unit: survey of behaviors and attitudes of 1384 healthcare professionals. Crit Care Med. 2009;37(3):825–32. https://doi.org/10.1097/CCM.0b013e31819b8608.
Woien H, Bjork IT. Intensive care pain treatment and sedation: nurses' experiences of the conflict between clinical judgement and standardised care: an explorative study. Intens Crit Care Nurs. 2013;29(3):128–36. https://doi.org/10.1016/j.iccn.2012.11.003.
Woien H, Stubhaug A, Bjork IT. Analgesia and sedation of mechanically ventilated patients - a national survey of clinical practice. Acta Anaesthesiol Scand. 2012;56(1):23–9. https://doi.org/10.1111/j.1399-6576.2011.02524.x.
Lewis-Newby M, Curtis JR, Martin DP, Engelberg RA. Measuring family satisfaction with care and quality of dying in the intensive care unit: does patient age matter? J Palliat Med. 2011;14(12):1284–90. https://doi.org/10.1089/jpm.2011.0138.
Osborn TR, Curtis JR, Nielsen EL, Back AL, Shannon SE, Engelberg RA. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control, and ICU atmosphere. Chest. 2012;142(5):1185–92. https://doi.org/10.1378/chest.11-3277.
Kodali S, Stametz RA, Bengier AC, Clarke DN, Layon AJ, Darer JD. Family experience with intensive care unit care: association of self-reported family conferences and family satisfaction. J Crit Care. 2014;29(4):641–4. https://doi.org/10.1016/j.jcrc.2014.03.012.
Rothen HU, Stricker KH, Heyland DK. Family satisfaction with critical care: measurements and messages. Curr Opin Crit Care. 2010;16(6):623–31. https://doi.org/10.1097/MCC.0b013e32833e9718.
Donabedian A. An introduction to quality assurance in health care. New York: Oxford University Press; 2003. xiii, 200 p. p.
Carlson EB, Spain DA, Muhtadie L, McDade-Montez L, Macia KS. Care and caring in the intensive care unit: family members' distress and perceptions about staff skills, communication, and emotional support. J Crit Care. 2015;30(3):557–61. https://doi.org/10.1016/j.jcrc.2015.01.012.
Dodek PM, Heyland DK, Rocker GM, Cook DJ. Translating family satisfaction data into quality improvement. Crit Care Med. 2004;32(9):1922–7. https://doi.org/10.1097/01.ccm.0000139920.53790.61.
Lind R, Lorem GF, Nortvedt P, Hevroy O. Intensive care nurses' involvement in the end-of-life process--perspectives of relatives. Nurs Ethics. 2012;19(5):666–76. https://doi.org/10.1177/0969733011433925.
The Act of July 2, 1999 No. 64 on Health Personnel (Health Personnel Act), §10 Information to patients. [Norwegian] 1999 [cited 2020 19.06]. Available from: https://lovdata.no/dokument/NL/lov/1999-07-02-64. Accessed 11 Feb 2021.
Acknowledgements
We thank the Norwegian Intensive Care Registry (NICR) for granting access to the data material.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
The study was conceptualized and conducted by ROH, HHB and AS. The statistical analysis was performed by ROH, HHB and AS, and the manuscript was written by ROH, HHB and AS. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participation
This study was approved by Norwegian Intensive Care Registry (NICR) and the data protection officer at the hospitals included. No other ethical approval was necessary since the family members answered the questionnaire anonymously. Returned questionnaires were regarded as written informed consent. The Norwegian Data Protection Authority approved the national FSICU project (number 2009/7537) carried out by NICR and Centre for Clinical Documentation and Evaluation (CCDE).
Consent of publication
Not applicable.
Competing interests
The authors declare no conflicts of interest with respect to the research, authorship and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Haave, R.O., Bakke, H.H. & Schröder, A. Family satisfaction in the intensive care unit, a cross-sectional study from Norway. BMC Emerg Med 21, 20 (2021). https://doi.org/10.1186/s12873-021-00412-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-021-00412-8